peptic ulcer disease
|
|
* From the American College of Gastroenterology Website
* Please scroll down for video discussion and more information on ulcer, bleeding, pain medications
OVERVIEW
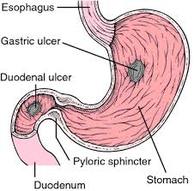
An “ulcer” is an open sore. The word “peptic” means that the cause of the problem is due to acid. Most of the time when a gastroenterologist is referring to an “ulcer” the doctor means a peptic ulcer.
The two most common types of peptic ulcer are called “gastric ulcers” and “duodenal ulcers”. These names refer to the location where the ulcer is found. Gastric ulcers are located in the stomach. Duodenal ulcers are found at the beginning of the small intestine (also called the small bowel) known as the duodenum. A person may have both gastric and duodenal ulcers at the same time.
SYMPTOMS
Many people with ulcers have no symptoms at all. Some people with an ulcer have belly pain. This pain is often in the upper abdomen. Sometimes food makes the pain better, and sometimes it makes it worse. Other symptoms include nausea, vomiting, or feeling bloated or full. It is important to know that there are many causes of abdominal pain, so not all pain in the abdomen is an “ulcer”.
The most important symptoms that ulcers cause are related to bleeding.
Bleeding from an ulcer can be slow and go unnoticed or can cause life-threatening hemorrhage. Ulcers that bleed slowly might not produce the symptoms until the person becomes anemic. Symptoms of anemia include fatigue, shortness of breath with exercise and pale skin color.
Bleeding that occurs more rapidly might show up as melena – jet black, very sticky stool (often compared to “roof tar”) – or even a large amount of dark red or maroon blood in the stool. People with bleeding ulcers may also vomit. This vomit may be red blood or may look like “coffee grounds”. Other symptoms might include “passing out” or feeling lightheaded. Symptoms of rapid bleeding represent a medical emergency. If this occurs, immediate medical attention is needed.
CAUSES & RISK FACTORS
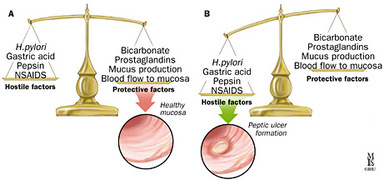
The two most important causes of ulcers are infection with Helicobacter pylori and a group of medications known as NSAIDs.
Helicobacter pylori (also called H. pylori or “HP) is a bacterium that lives in the stomach of infected people. The understanding that H. pylori can cause ulcers was one of the most important medical discoveries of the late 20th century.
People infected with H. pylori are at increased risk of developing peptic ulcers. When a person is diagnosed with an ulcer, testing for H. pylori is often done. There are a number of tests to diagnose H. pylori and the type of test used depends on the situation.
People with ulcers. who are infected with H. pylori. should have their infection treated. Treatment usually consists of taking either three or four drugs. The drug therapy will use acid suppression therapy with a proton pump inhibitor (PPI) along with antibiotic therapy and perhaps a bismuth containing agent such as Pepto-Bismol. H. pylori can be very difficult to cure; so it is very important that people being treated for this infection take their entire course of antibiotics as prescribed.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) are a group of medications typically used to treat pain. There are many drugs in this group. A few of these include: aspirin (Bayer®), ibuprofen (Motrin®, Advil®), naproxen (Aleve®, Naprosyn®), ketorolac (Toradol®) and oxaprozin (Daypro®). NSAIDs are also included in some combination medications, such as Alka-Seltzer®, Goody’s Powder® and BC Powder®.
NSAID use is very common because many are available over the counter without a prescriptionand therefore they are a very common cause of peptic ulcers. NSAIDs cause ulcers by interrupting the natural ability of the stomach and the duodenum to protect themselves from stomach acid. NSAIDs also can interfere with blood clotting, which has obvious importance when ulcers bleed.
People who take NSAIDs for a long time and/or at high doses, have a higher risk of developing ulcers. These people should discuss the various options for preventing ulcers with their physician. Some people are given an acid suppressing PPI. These drugs can prevent or significantly reduce the risk of an ulcer being caused by NSAIDs.
DIAGNOSIS
The most typical way for ulcers to be diagnosed is by a procedure called an EGD. EGD stands forEsophagoGastroDuodenoscopy. An EGD (also called “upper endoscopy”) is performed by inserting a special lighted camera on a flexible tube into the person’s mouth to look directly into the stomach and the beginning of the small bowel. This flexible camera carefully inspects the most likely areas for ulcers to be located. Ulcers identified during an EGD may be photographed, biopsied and even treated, if bleeding is present.
TREATMENT
The way that ulcers are treated depends on a number of features. Nearly all peptic ulcers will be treated with a proton pump inhibitor (PPI). PPIs are powerful acid blocking drugs that can be taken as a pill or given in an IV. Often, the potent IV form is used if a patient is hospitalized with a bleeding ulcer.
PPIs require a meal to activate them. Patients should eat a meal within 30 minutes to 1 hour after taking this medication for the acid suppression therapy to work most effectively. Waiting later than this time can decrease the positive effect of this medication. This might delay healing or even result in the failure of the ulcer to heal.
Sometimes duodenal ulcers (not gastric ulcers) will be treated with H2 blockers. H2 blockers are another type of acid reducing medication.
An important part in treating ulcers is by identifying what caused them Patients with ulcers caused by NSAIDs should talk to their doctor about other medications that can be used to treat pain.
If the person is infected with H. pylori this infection should be treated. Completing the full dose of antibiotics is very important. Just as important, is making sure that the infection is gone. There are number of ways to do this. Generally, a blood test is not a good way to test if the infection is gone. The doctor who treated the infection can recommend the best way to do the “test of cure”.
When someone has an ulcer that has bled significantly, treatment might be done at the time of EGD. There are a number of techniques that can be performed during an EGD to control bleeding from an ulcer. The gastroenterologist might inject medications, use a catheter to cauterize the ulcer (burn a bleeding vessel shut) or place a small clip to clamp off a bleeding vessel. Not all ulcers need to be treated this way. The doctor doing the EGD will decide if treatment is indicated based on the way the ulcer looks. The doctor will usually treat an ulcer that is actually bleeding when it is seen and will also often treat other ulcers if they have a certain appearance. These findings are sometimes called “stigmata of recent hemorrhage” or just “stigmata”. Stigmata will usually get treated during the EGD if they are classified as high-risk. Common high-risk findings include a “visible vessel” and an “adherent clot”.
Most ulcers can be treated and will heal. Often, people with ulcers will have to take PPIs for several weeks to heal an ulcer. It is also important to correct what caused the ulcer. When possible, NSAIDs should be stopped. Patients with ulcers caused by NSAIDs should talk to their doctor about other medications that can be used to treat pain.
* Please scroll down for video discussion and more information on ulcer, bleeding, pain medications
OVERVIEW
An “ulcer” is an open sore. The word “peptic” means that the cause of the problem is due to acid. Most of the time when a gastroenterologist is referring to an “ulcer” the doctor means a peptic ulcer.
The two most common types of peptic ulcer are called “gastric ulcers” and “duodenal ulcers”. These names refer to the location where the ulcer is found. Gastric ulcers are located in the stomach. Duodenal ulcers are found at the beginning of the small intestine (also called the small bowel) known as the duodenum. A person may have both gastric and duodenal ulcers at the same time.
SYMPTOMS
Many people with ulcers have no symptoms at all. Some people with an ulcer have belly pain. This pain is often in the upper abdomen. Sometimes food makes the pain better, and sometimes it makes it worse. Other symptoms include nausea, vomiting, or feeling bloated or full. It is important to know that there are many causes of abdominal pain, so not all pain in the abdomen is an “ulcer”.
The most important symptoms that ulcers cause are related to bleeding.
Bleeding from an ulcer can be slow and go unnoticed or can cause life-threatening hemorrhage. Ulcers that bleed slowly might not produce the symptoms until the person becomes anemic. Symptoms of anemia include fatigue, shortness of breath with exercise and pale skin color.
Bleeding that occurs more rapidly might show up as melena – jet black, very sticky stool (often compared to “roof tar”) – or even a large amount of dark red or maroon blood in the stool. People with bleeding ulcers may also vomit. This vomit may be red blood or may look like “coffee grounds”. Other symptoms might include “passing out” or feeling lightheaded. Symptoms of rapid bleeding represent a medical emergency. If this occurs, immediate medical attention is needed.
CAUSES & RISK FACTORS
The two most important causes of ulcers are infection with Helicobacter pylori and a group of medications known as NSAIDs.
Helicobacter pylori (also called H. pylori or “HP) is a bacterium that lives in the stomach of infected people. The understanding that H. pylori can cause ulcers was one of the most important medical discoveries of the late 20th century.
People infected with H. pylori are at increased risk of developing peptic ulcers. When a person is diagnosed with an ulcer, testing for H. pylori is often done. There are a number of tests to diagnose H. pylori and the type of test used depends on the situation.
People with ulcers. who are infected with H. pylori. should have their infection treated. Treatment usually consists of taking either three or four drugs. The drug therapy will use acid suppression therapy with a proton pump inhibitor (PPI) along with antibiotic therapy and perhaps a bismuth containing agent such as Pepto-Bismol. H. pylori can be very difficult to cure; so it is very important that people being treated for this infection take their entire course of antibiotics as prescribed.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) are a group of medications typically used to treat pain. There are many drugs in this group. A few of these include: aspirin (Bayer®), ibuprofen (Motrin®, Advil®), naproxen (Aleve®, Naprosyn®), ketorolac (Toradol®) and oxaprozin (Daypro®). NSAIDs are also included in some combination medications, such as Alka-Seltzer®, Goody’s Powder® and BC Powder®.
NSAID use is very common because many are available over the counter without a prescriptionand therefore they are a very common cause of peptic ulcers. NSAIDs cause ulcers by interrupting the natural ability of the stomach and the duodenum to protect themselves from stomach acid. NSAIDs also can interfere with blood clotting, which has obvious importance when ulcers bleed.
People who take NSAIDs for a long time and/or at high doses, have a higher risk of developing ulcers. These people should discuss the various options for preventing ulcers with their physician. Some people are given an acid suppressing PPI. These drugs can prevent or significantly reduce the risk of an ulcer being caused by NSAIDs.
DIAGNOSIS
The most typical way for ulcers to be diagnosed is by a procedure called an EGD. EGD stands forEsophagoGastroDuodenoscopy. An EGD (also called “upper endoscopy”) is performed by inserting a special lighted camera on a flexible tube into the person’s mouth to look directly into the stomach and the beginning of the small bowel. This flexible camera carefully inspects the most likely areas for ulcers to be located. Ulcers identified during an EGD may be photographed, biopsied and even treated, if bleeding is present.
TREATMENT
The way that ulcers are treated depends on a number of features. Nearly all peptic ulcers will be treated with a proton pump inhibitor (PPI). PPIs are powerful acid blocking drugs that can be taken as a pill or given in an IV. Often, the potent IV form is used if a patient is hospitalized with a bleeding ulcer.
PPIs require a meal to activate them. Patients should eat a meal within 30 minutes to 1 hour after taking this medication for the acid suppression therapy to work most effectively. Waiting later than this time can decrease the positive effect of this medication. This might delay healing or even result in the failure of the ulcer to heal.
Sometimes duodenal ulcers (not gastric ulcers) will be treated with H2 blockers. H2 blockers are another type of acid reducing medication.
An important part in treating ulcers is by identifying what caused them Patients with ulcers caused by NSAIDs should talk to their doctor about other medications that can be used to treat pain.
If the person is infected with H. pylori this infection should be treated. Completing the full dose of antibiotics is very important. Just as important, is making sure that the infection is gone. There are number of ways to do this. Generally, a blood test is not a good way to test if the infection is gone. The doctor who treated the infection can recommend the best way to do the “test of cure”.
When someone has an ulcer that has bled significantly, treatment might be done at the time of EGD. There are a number of techniques that can be performed during an EGD to control bleeding from an ulcer. The gastroenterologist might inject medications, use a catheter to cauterize the ulcer (burn a bleeding vessel shut) or place a small clip to clamp off a bleeding vessel. Not all ulcers need to be treated this way. The doctor doing the EGD will decide if treatment is indicated based on the way the ulcer looks. The doctor will usually treat an ulcer that is actually bleeding when it is seen and will also often treat other ulcers if they have a certain appearance. These findings are sometimes called “stigmata of recent hemorrhage” or just “stigmata”. Stigmata will usually get treated during the EGD if they are classified as high-risk. Common high-risk findings include a “visible vessel” and an “adherent clot”.
Most ulcers can be treated and will heal. Often, people with ulcers will have to take PPIs for several weeks to heal an ulcer. It is also important to correct what caused the ulcer. When possible, NSAIDs should be stopped. Patients with ulcers caused by NSAIDs should talk to their doctor about other medications that can be used to treat pain.
|
|
|
