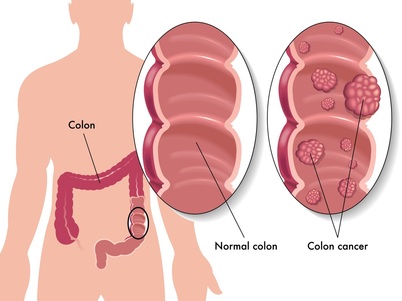
COLON CANCER
http://www.uptodate.com Miguel A Rodriguez-Bigas, MD, Axel Grothey, MD
Please scroll down for more information, videos,illustrations.
COLORECTAL CANCER SYMPTOMS — The most common symptoms of colon and rectal cancer include:
●Stomach pain or frequent gas pains
●Change in bowel habits (constipation or diarrhea)
●Blood in the bowel movements
●Feeling weak or tired
●Low iron level (iron deficiency anemia)
●Black or dark-colored stools
COLORECTAL CANCER DIAGNOSIS — Your doctor or nurse may be concerned that you could have colon or rectal cancer if you have one or more of the above symptoms. In this case, a colonoscopy is often used to look inside the rectum and large intestine. Cancers growing within the large intestine and rectum can be seen during a colonoscopy, and a biopsy (removal of a piece of tissue for examination) can be done, confirming the presence of a cancer. Colonoscopy is described in a separate article.
Staging — Once a colorectal cancer is diagnosed, the next step is to determine its stage. Staging is a system used to describe the aggressiveness and spread of a cancer. The stage of a colorectal cancer is assigned based on:
●Whether there are signs of cancer spread on a physical exam, CT scan, or MRI of the abdomen and pelvis, chest X-ray, or other imaging tests.
●The appearance of the cancer specimen when viewed under the microscope, after it has been removed with surgery.
Colorectal cancer stages range from stage I (cancer has invaded into but not through the entire wall of the intestine), to stage IV (the cancer has spread to distant organs, such as the liver). Treatment depends on disease stage.
Earlier stages of disease (stages I through III) are referred to as localized colorectal cancers and generally treated with surgery, with or without chemotherapy.
Stage IV cancer is called advanced colorectal cancer and is generally treated with chemotherapy; some patients may benefit from surgery of the primary tumor and sometimes of metastases. Treatment of stage IV disease is covered elsewhere.
COLON CANCER TREATMENT — The treatment of colon cancer usually involves surgery, and it may also involve chemotherapy; radiation therapy is only rarely needed.
Surgery — The initial treatment of colon cancer usually involves surgery.
During the surgery, the cancerous part of the colon and surrounding tissues are removed. The lymph nodes (round organs that serve as filters for blood from the intestines) within this surrounding tissue are examined under a microscope to determine if the cancer has spread beyond the colon.
In most people, the two ends of the colon can be reconnected immediately after the cancerous part has been removed. If this can be done, it means that you will continue to have bowel movements normally, through your rectum and anus.
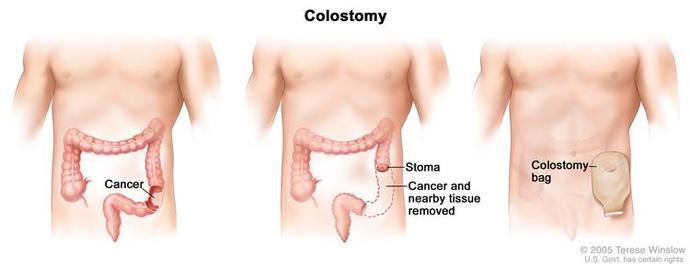
In other cases, the colon cannot be reconnected during the initial surgery. This can happen if the surgeon feels there is a high chance that the reconnection will fail or if the tissues are inflamed and need time to heal. If this occurs, the surgeon will sew the colon (and at times the small bowel) to an opening in the skin on the abdomen. The opening is called an ostomy (colostomy if the colon is sewn to the abdominal wall or ileostomy if the ileum is sewn to the abdominal wall). You will wear a bag over the ostomy to collect bowel movements.
The ostomy is usually temporary. The two ends of the colon can often be reconnected after a few months, sometimes after chemotherapy is completed. In other cases, you will need the colostomy permanently.
Life with a colostomy — Having a colostomy will change how your body looks, which can be hard to accept. However, with education and support, it is possible to lead an active life with a colostomy. A team effort, which includes the colorectal surgeon, oncologist, and an enterostomal therapy (ET) nurse, is valuable in learning about the surgery and also in the care and recovery required after the procedure. The United Ostomy Associations of America is also a good source of information and support (www.uoaa.org).
Chemotherapy — Chemotherapy is a treatment given to slow or stop the growth of cancer cells. Even after a colon cancer has been completely removed with surgery, cancer cells can remain in the body, increasing the risk of the cancer coming back (called a relapse or recurrence). In some people, chemotherapy can eliminate these cancer cells and increase the chance of cure. This type of chemotherapy is called "adjuvant", which means that it is given after a curative surgery (at which time all the tumor was removed).
Most treatments involve a combination of several chemotherapy drugs, which are given in a specific order on specific days. Most of the drugs are given into the vein (intravenous, IV), but sometimes a single drug will be recommended, which can be given in pill form. Regardless of the specific type of regimen, most adjuvant treatment regimens for colon cancer last about six months.
Your healthcare provider can describe which chemotherapy drugs will be needed, how long treatment will last, and what side effects are expected from your treatment.
Who needs chemotherapy? — Chemotherapy is recommended for most people with stage III colon cancer (spread to the lymph nodes) and some people with stage II colon cancer (involvement of the whole thickness of the bowel wall but without involvement of the lymph nodes). Chemotherapy is not recommended for people with stage I colon cancer (cancer within the bowel wall but not all the way through it).
Before you begin chemotherapy, it is important to discuss the potential risks and benefits of treatment with your doctor.
●In some cases, the benefits of chemotherapy (better chance of survival) clearly outweigh the possible risks (chemotherapy side effects like diarrhea, vomiting, hair loss, nerve damage, or more serious risks). Not everyone will have all of these side effects.
●In other cases, the benefit of chemotherapy is not worth the risks.
RECTAL CANCER TREATMENT — The majority of rectal cancers are treated with a combination of surgery, radiation therapy, and chemotherapy; as with colon cancers, treatment is chosen based upon disease stage.
●Stage I rectal cancer — Surgery alone may cure the cancer.
●Stage II and III — Chemotherapy and radiation therapy are typically recommended along with surgery; in general, the chemotherapy and radiation are given before surgery (referred to as neoadjuvant chemoradiotherapy), with additional chemotherapy given after surgery.
●Stage IV — Predominantly treated with chemotherapy, with or without surgery.
Neoadjuvant chemoradiotherapy and radiotherapy — A combination of chemotherapy and radiation therapy may be recommended before surgery for patients with rectal cancer; this is called neoadjuvant chemoradiotherapy. This treatment can shrink the tumor before it is removed, reduces the risk that the cancer will come back, and may reduce the chances that you will need a permanent colostomy.
The two most common ways to take chemotherapy during radiation therapy are:
●A pump that fits into a pack you wear around your waist. The pump delivers the medicine (called 5-FU) into a port (an IV in your chest) continuously for about six weeks during radiation treatments.
●Daily doses of a pill called capecitabine on the days of radiation treatment. The pill is as effective as 5-FU given by pump and more convenient.
●Discuss all the potential risks and benefits of capecitabine with your doctor.
In some cases, a short course of radiation therapy alone (typically five daily treatments) may be recommended prior to surgery instead of combined chemotherapy and radiation. This approach is more popular outside of the United States.
Surgery — Surgery removes the cancerous part of the rectum and the associated lymph nodes. Sometimes this will require that the anus be removed along with the rectum. If the anus and rectum have to be removed, the surgeon will sew the remaining intestine to an opening in the skin on the abdomen. The opening is called a colostomy. You will wear a bag over the opening to collect bowel movements.
The type of surgery you have depends upon where your tumor is located and how far it has spread. Another factor to consider is your current bowel function specifically how well you control your bowels. Ask your surgeon to describe which surgery is right for you.
Treatment after surgery — Postoperative (adjuvant) therapy is typically recommended after surgery. The type of treatment you have after surgery depends upon the stage of your cancer, as well as the treatment you had before surgery. (See "Adjuvant therapy for resected rectal adenocarcinoma".)
●If your tumor is stage II or III, and you did not have chemotherapy and radiation therapy before surgery, you will probably have it after surgery. This is called adjuvant chemoradiotherapy (see 'Neoadjuvant chemoradiotherapy and radiotherapy' above).
●If you had chemoradiotherapy or radiation therapy alone before surgery, you will probably need approximately four to six months of chemotherapy alone (without further radiation therapy) after surgery.
FOLLOW-UP AFTER TREATMENT — After completing treatment for colorectal cancer, it is important to follow up with your healthcare team. You will need appointments on a regular basis for a few years to monitor for signs that the cancer has recurred.
Several expert groups have issued guidelines for follow-up after treatment for a colorectal cancer, and they all differ slightly. Most people will have the following:
●A full colonoscopy before or after surgery to look for polyps or other cancers that were not seen previously. Colonoscopy is usually repeated one year after surgery, and if this is normal, then every three to five years thereafter. If polyps or new cancers are found, this schedule may be adjusted.
For patients with rectal cancer who have undergone limited surgery (eg, removal of the cancerous tumor only) or standard surgery without radiation therapy, more frequent follow-up exams are recommended for the first two to three years. These involve a proctosigmoidoscopy (which is similar to a colonoscopy but only looks at the lower part of the colon) and may or may not involve an endoscopic ultrasound (which is also done by inserting a scope but uses sound waves to produce images of the rectum).
●Visits with your healthcare provider are usually scheduled every three to four months for the first two to three years, then every six months for two years. Most visits will include a discussion of how you are feeling and a physical examination. A blood test for a colorectal cancer tumor marker (CEA) may be done at each visit.
●A CT scan is usually recommended once per year for at least three years in people who have been treated for stage II or III colon cancer.
COLORECTAL CANCER AND YOUR FAMILY — Having colon or rectal cancer means that your family may be at an increased risk of developing colorectal cancer. If you have one parent, brother, sister, or child with colorectal cancer or polyps at a young age (before the age of 60 years), or two relatives diagnosed at any age, you should begin screening for colon cancer earlier, typically at age 40, or 10 years younger than the earliest diagnosis in your family, whichever comes first. Colon cancer screening is discussed separately.
Certain genetic conditions increase the risk of colon cancer. The most common conditions include Lynch syndrome (also called hereditary nonpolyposis colon cancer, HNPCC), and familial adenomatous polyposis (FAP). If you have a strong family history of colon cancer (two or more close relatives), talk to your doctor about the need for genetic counseling and possible genetic testing.Although the idea of genetic testing can be frightening, the results of genetic tests can help determine whether you and your family need further treatment, testing, or closer surveillance.
WHERE TO GET MORE INFORMATION — Your healthcare provider is the best source of information for questions and concerns related to your medical problem.
Please scroll down for more information, videos,illustrations.
COLORECTAL CANCER SYMPTOMS — The most common symptoms of colon and rectal cancer include:
●Stomach pain or frequent gas pains
●Change in bowel habits (constipation or diarrhea)
●Blood in the bowel movements
●Feeling weak or tired
●Low iron level (iron deficiency anemia)
●Black or dark-colored stools
COLORECTAL CANCER DIAGNOSIS — Your doctor or nurse may be concerned that you could have colon or rectal cancer if you have one or more of the above symptoms. In this case, a colonoscopy is often used to look inside the rectum and large intestine. Cancers growing within the large intestine and rectum can be seen during a colonoscopy, and a biopsy (removal of a piece of tissue for examination) can be done, confirming the presence of a cancer. Colonoscopy is described in a separate article.
Staging — Once a colorectal cancer is diagnosed, the next step is to determine its stage. Staging is a system used to describe the aggressiveness and spread of a cancer. The stage of a colorectal cancer is assigned based on:
●Whether there are signs of cancer spread on a physical exam, CT scan, or MRI of the abdomen and pelvis, chest X-ray, or other imaging tests.
●The appearance of the cancer specimen when viewed under the microscope, after it has been removed with surgery.
Colorectal cancer stages range from stage I (cancer has invaded into but not through the entire wall of the intestine), to stage IV (the cancer has spread to distant organs, such as the liver). Treatment depends on disease stage.
Earlier stages of disease (stages I through III) are referred to as localized colorectal cancers and generally treated with surgery, with or without chemotherapy.
Stage IV cancer is called advanced colorectal cancer and is generally treated with chemotherapy; some patients may benefit from surgery of the primary tumor and sometimes of metastases. Treatment of stage IV disease is covered elsewhere.
COLON CANCER TREATMENT — The treatment of colon cancer usually involves surgery, and it may also involve chemotherapy; radiation therapy is only rarely needed.
Surgery — The initial treatment of colon cancer usually involves surgery.
During the surgery, the cancerous part of the colon and surrounding tissues are removed. The lymph nodes (round organs that serve as filters for blood from the intestines) within this surrounding tissue are examined under a microscope to determine if the cancer has spread beyond the colon.
In most people, the two ends of the colon can be reconnected immediately after the cancerous part has been removed. If this can be done, it means that you will continue to have bowel movements normally, through your rectum and anus.
In other cases, the colon cannot be reconnected during the initial surgery. This can happen if the surgeon feels there is a high chance that the reconnection will fail or if the tissues are inflamed and need time to heal. If this occurs, the surgeon will sew the colon (and at times the small bowel) to an opening in the skin on the abdomen. The opening is called an ostomy (colostomy if the colon is sewn to the abdominal wall or ileostomy if the ileum is sewn to the abdominal wall). You will wear a bag over the ostomy to collect bowel movements.
The ostomy is usually temporary. The two ends of the colon can often be reconnected after a few months, sometimes after chemotherapy is completed. In other cases, you will need the colostomy permanently.
Life with a colostomy — Having a colostomy will change how your body looks, which can be hard to accept. However, with education and support, it is possible to lead an active life with a colostomy. A team effort, which includes the colorectal surgeon, oncologist, and an enterostomal therapy (ET) nurse, is valuable in learning about the surgery and also in the care and recovery required after the procedure. The United Ostomy Associations of America is also a good source of information and support (www.uoaa.org).
Chemotherapy — Chemotherapy is a treatment given to slow or stop the growth of cancer cells. Even after a colon cancer has been completely removed with surgery, cancer cells can remain in the body, increasing the risk of the cancer coming back (called a relapse or recurrence). In some people, chemotherapy can eliminate these cancer cells and increase the chance of cure. This type of chemotherapy is called "adjuvant", which means that it is given after a curative surgery (at which time all the tumor was removed).
Most treatments involve a combination of several chemotherapy drugs, which are given in a specific order on specific days. Most of the drugs are given into the vein (intravenous, IV), but sometimes a single drug will be recommended, which can be given in pill form. Regardless of the specific type of regimen, most adjuvant treatment regimens for colon cancer last about six months.
Your healthcare provider can describe which chemotherapy drugs will be needed, how long treatment will last, and what side effects are expected from your treatment.
Who needs chemotherapy? — Chemotherapy is recommended for most people with stage III colon cancer (spread to the lymph nodes) and some people with stage II colon cancer (involvement of the whole thickness of the bowel wall but without involvement of the lymph nodes). Chemotherapy is not recommended for people with stage I colon cancer (cancer within the bowel wall but not all the way through it).
Before you begin chemotherapy, it is important to discuss the potential risks and benefits of treatment with your doctor.
●In some cases, the benefits of chemotherapy (better chance of survival) clearly outweigh the possible risks (chemotherapy side effects like diarrhea, vomiting, hair loss, nerve damage, or more serious risks). Not everyone will have all of these side effects.
●In other cases, the benefit of chemotherapy is not worth the risks.
RECTAL CANCER TREATMENT — The majority of rectal cancers are treated with a combination of surgery, radiation therapy, and chemotherapy; as with colon cancers, treatment is chosen based upon disease stage.
●Stage I rectal cancer — Surgery alone may cure the cancer.
●Stage II and III — Chemotherapy and radiation therapy are typically recommended along with surgery; in general, the chemotherapy and radiation are given before surgery (referred to as neoadjuvant chemoradiotherapy), with additional chemotherapy given after surgery.
●Stage IV — Predominantly treated with chemotherapy, with or without surgery.
Neoadjuvant chemoradiotherapy and radiotherapy — A combination of chemotherapy and radiation therapy may be recommended before surgery for patients with rectal cancer; this is called neoadjuvant chemoradiotherapy. This treatment can shrink the tumor before it is removed, reduces the risk that the cancer will come back, and may reduce the chances that you will need a permanent colostomy.
The two most common ways to take chemotherapy during radiation therapy are:
●A pump that fits into a pack you wear around your waist. The pump delivers the medicine (called 5-FU) into a port (an IV in your chest) continuously for about six weeks during radiation treatments.
●Daily doses of a pill called capecitabine on the days of radiation treatment. The pill is as effective as 5-FU given by pump and more convenient.
●Discuss all the potential risks and benefits of capecitabine with your doctor.
In some cases, a short course of radiation therapy alone (typically five daily treatments) may be recommended prior to surgery instead of combined chemotherapy and radiation. This approach is more popular outside of the United States.
Surgery — Surgery removes the cancerous part of the rectum and the associated lymph nodes. Sometimes this will require that the anus be removed along with the rectum. If the anus and rectum have to be removed, the surgeon will sew the remaining intestine to an opening in the skin on the abdomen. The opening is called a colostomy. You will wear a bag over the opening to collect bowel movements.
The type of surgery you have depends upon where your tumor is located and how far it has spread. Another factor to consider is your current bowel function specifically how well you control your bowels. Ask your surgeon to describe which surgery is right for you.
Treatment after surgery — Postoperative (adjuvant) therapy is typically recommended after surgery. The type of treatment you have after surgery depends upon the stage of your cancer, as well as the treatment you had before surgery. (See "Adjuvant therapy for resected rectal adenocarcinoma".)
●If your tumor is stage II or III, and you did not have chemotherapy and radiation therapy before surgery, you will probably have it after surgery. This is called adjuvant chemoradiotherapy (see 'Neoadjuvant chemoradiotherapy and radiotherapy' above).
●If you had chemoradiotherapy or radiation therapy alone before surgery, you will probably need approximately four to six months of chemotherapy alone (without further radiation therapy) after surgery.
FOLLOW-UP AFTER TREATMENT — After completing treatment for colorectal cancer, it is important to follow up with your healthcare team. You will need appointments on a regular basis for a few years to monitor for signs that the cancer has recurred.
Several expert groups have issued guidelines for follow-up after treatment for a colorectal cancer, and they all differ slightly. Most people will have the following:
●A full colonoscopy before or after surgery to look for polyps or other cancers that were not seen previously. Colonoscopy is usually repeated one year after surgery, and if this is normal, then every three to five years thereafter. If polyps or new cancers are found, this schedule may be adjusted.
For patients with rectal cancer who have undergone limited surgery (eg, removal of the cancerous tumor only) or standard surgery without radiation therapy, more frequent follow-up exams are recommended for the first two to three years. These involve a proctosigmoidoscopy (which is similar to a colonoscopy but only looks at the lower part of the colon) and may or may not involve an endoscopic ultrasound (which is also done by inserting a scope but uses sound waves to produce images of the rectum).
●Visits with your healthcare provider are usually scheduled every three to four months for the first two to three years, then every six months for two years. Most visits will include a discussion of how you are feeling and a physical examination. A blood test for a colorectal cancer tumor marker (CEA) may be done at each visit.
●A CT scan is usually recommended once per year for at least three years in people who have been treated for stage II or III colon cancer.
COLORECTAL CANCER AND YOUR FAMILY — Having colon or rectal cancer means that your family may be at an increased risk of developing colorectal cancer. If you have one parent, brother, sister, or child with colorectal cancer or polyps at a young age (before the age of 60 years), or two relatives diagnosed at any age, you should begin screening for colon cancer earlier, typically at age 40, or 10 years younger than the earliest diagnosis in your family, whichever comes first. Colon cancer screening is discussed separately.
Certain genetic conditions increase the risk of colon cancer. The most common conditions include Lynch syndrome (also called hereditary nonpolyposis colon cancer, HNPCC), and familial adenomatous polyposis (FAP). If you have a strong family history of colon cancer (two or more close relatives), talk to your doctor about the need for genetic counseling and possible genetic testing.Although the idea of genetic testing can be frightening, the results of genetic tests can help determine whether you and your family need further treatment, testing, or closer surveillance.
WHERE TO GET MORE INFORMATION — Your healthcare provider is the best source of information for questions and concerns related to your medical problem.
|
|
|