pancreatic cancer
http://www.uptodate.com David P Ryan, MD
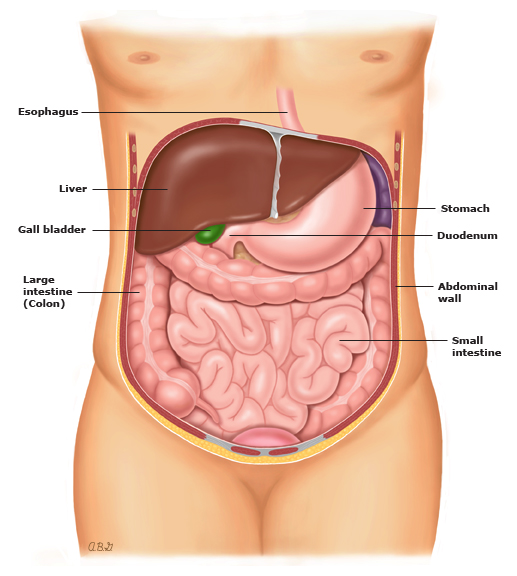
INTRODUCTION — The pancreas is an organ that is located behind the stomach. Its normal function is to make hormones that regulate glucose (blood sugar) levels and produce digestive juices that help the body break down food.
More than 42,000 Americans develop cancer of the pancreas each year; it is the fourth leading cause of cancer-related death in the United States. Two types of cancer can affect the pancreas:
●The most common is cancer of the exocrine pancreas that originates in the pancreatic ducts. The ducts are responsible for carrying pancreatic juice to the intestines. This type of pancreatic cancer, called "pancreatic ductal adenocarcinoma," is discussed in this article.
●Another type of cancer consists of a group of tumors that originate from the cells that make hormones such as insulin. These tumors are called "pancreatic endocrine tumors," and are not discussed here.
PANCREATIC CANCER SYMPTOMS — Most people with pancreatic cancer have pain and weight loss, with or without jaundice (yellowing of the skin):
●Pain – Pain is a common symptom. It usually develops in the upper abdomen as a dull ache that wraps around to the back. The pain can come and go, and it might get worse after eating.
●Weight loss – Some people lose weight because of a lack of appetite, feeling full after eating only a small amount of food, or having diarrhea. The bowel movements might look greasy and float in the toilet bowl because they contain undigested fat.
●Jaundice – This causes yellow colored skin and whites of the eyes. Bowel movements may not be a normal brown color and instead have a grayish appearance. Jaundice is caused by a block in the flow of bile from the gallbladder, where it is stored, to the intestinal tract where the bile assists in digestion of food. The block is caused by the cancer.
PANCREATIC CANCER DIAGNOSIS — If you develop symptoms that raise suspicion for pancreatic cancer, your doctor or nurse will order one or more tests. These might include blood tests and imaging tests, such as an ultrasound or computed tomography (CT) scan, and/or an endoscopic test called endoscopic retrograde cholangiopancreatography (ERCP).
These tests can show if there is a mass (growth) in the pancreas and if surgery to remove the mass is possible.
Biopsy — In some cases, your doctor will recommend a biopsy to confirm the diagnosis of cancer. A biopsy involves removing a small piece of tissue from the mass. A physician examines the tissue under a microscope to see if there are signs of cancer.
To perform the biopsy, a doctor will use a CT scan or ultrasound to pinpoint the location of the mass, then insert a needle into the mass and take a sample of tissue. A biopsy may also be obtained using ERCP or a different type of endoscopic procedure called endoscopic ultrasound (EUS).
PANCREATIC CANCER STAGING — Once pancreatic cancer is diagnosed, the next step is to determine its stage. Staging is a system used to describe the aggressiveness and spread of a cancer. A pancreatic cancer's stage is based on:
●The size of the cancer
●If there are signs of cancer spread outside the pancreas on a physical exam, computed tomography (CT) scan or magnetic resonance imaging (MRI), chest x-ray, or other imaging tests
The staging of a pancreatic cancer often depends not only on imaging studies, but also on what is found during surgery.
Pancreatic cancer stages range from stage I, the earliest stage, to stage IV, which means that the cancer has spread to distant organs (such as the liver). In general, lower stage cancers are more likely to be successfully treated than are higher stage cancers. Most physicians who care for patients with pancreatic cancer refer to patients as having surgically resectable cancer (stage I and II), locally advanced cancer (stage III), or metastatic cancer (stage IV).
Sometimes you will hear physicians describe a stage that technically doesn’t exist called "borderline resectable." This occurs because some locally advanced cancers can be resected completely, but many cannot. Imaging doesn’t always accurately distinguish between the two. In such cases, chemotherapy, with or without radiation therapy, might be used initially to attempt to shrink the tumor and increase the chance that it might become resectable.
Laparoscopy — In some centers, a laparoscopy is recommended before an attempt to remove the cancer surgically to get more information about the location and size of the cancer. During a laparoscopy, a surgeon inserts a thin tube with a camera into small incisions in the belly to see the organs inside the abdomen.
PANCREATIC CANCER TREATMENT — Pancreatic cancer can be treated with several approaches. Early stage pancreatic cancer can often be treated and even cured with surgery. After surgery, further treatment, called "adjuvant therapy," is often recommended. This might include chemotherapy or radiation therapy.
However, surgery is often not possible; pancreatic cancer is often advanced by the time it is diagnosed. If surgery is not possible, radiation therapy, chemotherapy, or both are often used to shrink the cancer, reduce symptoms, and prolong life.
Surgery for tumors in the head of the pancreas — The standard operation for tumors in the head of the pancreas is a Whipple procedure (also called a pancreaticoduodenectomy).
In this procedure, the surgeon removes the pancreatic head, the duodenum (the first part of the small intestine), part of the jejunum (the next part of the small intestine), the common bile duct, the gallbladder, and part of the stomach. A modification of the Whipple procedure (called a "pylorus-preserving" Whipple procedure) has been developed that preserves the part of the stomach (the pylorus) that is important for stomach emptying.
In the past, complications and deaths following the Whipple procedure were high, and cure rates were less than 10 percent. However, more recent results suggest better outcomes. Better outcomes are more likely in hospitals that perform a large number of Whipple procedures and when the surgeon is experienced with the procedure.
Surgery for tumors in the body or tail of the pancreas — Because tumors in the body or tail of the pancreas do not cause the same symptoms as those in the head of the pancreas, these cancers tend to be discovered at a later stage, when they are more advanced.
If the tumor can be removed with surgery, a laparoscopy is usually done first to make sure the cancer has not spread. If surgery is an option, part of the pancreas is removed, usually along with the spleen.
Adjuvant therapy after surgery — Adjuvant (additional) therapy refers to chemotherapy, radiation, or a combination of both. Adjuvant therapy is recommended for people who are thought to be at high-risk of having cancer reappear (termed a recurrence or a relapse) after a tumor has been removed surgically.
Even if the tumor has been completely removed, tiny cancer cells may remain in the body and grow, causing relapse after surgery. Adjuvant therapy can prolong survival by eliminating the tiny cancer cells before they have a chance to grow.
In people with completely resected pancreatic cancer, there are two ways to give adjuvant therapy after surgery:
●Give chemotherapy alone
●Give a combination of chemotherapy and radiation therapy (this strategy is called "chemoradiotherapy")
In the United States, after successful surgical removal of a pancreatic cancer, chemoradiotherapy is recommended for many patients, although chemotherapy alone is increasingly used. Outside of the United States, patients are frequently offered chemotherapy alone.
Treatment of locally advanced pancreatic cancer — Locally advanced pancreatic cancer refers to a situation in which the cancer has not yet spread to distant locations in the body, but it has extended into areas around the pancreas that make it difficult or impossible to remove the tumor completely. As determined by imaging studies (typically computed tomography [CT] and magnetic resonance imaging [MRI] scans), some of these cases may be classified as "borderline" resectable, while others are locally advanced and not resectable, according to standard guidelines.
The best treatment for locally advanced pancreatic cancer is not clear, but surgery is not usually offered initially. Options for treatment include chemotherapy alone or chemotherapy followed by a combination of chemotherapy and radiation therapy (chemoradiotherapy). In some cases, these treatments may be followed by repeat imaging and surgical exploration to see if tumor removal might be possible. Ideally, patients with locally advanced pancreatic cancer should be offered treatment as part of a clinical trial testing the benefit of new treatment strategies.
Chemoradiotherapy — Chemoradiotherapy often requires a central venous access catheter (often called a "port"). This is a tube that is surgically inserted into one of the large blood vessels in the chest. Chemoradiotherapy often requires a portable chemotherapy pump; this is a small, battery-operated pump that fits into a pack that can be worn around the waist. The pump gives the chemotherapy medicine into the port continuously for five to six weeks.
During this time, the patient is treated with radiation therapy five days per week. The radiation is delivered while the patient lies on a table underneath or in front of the machine. The treatment takes only a few seconds (similar to having an X-ray).
Sometimes the chemotherapy pump is not covered by health insurance. In this case, an oral (pill) form of chemotherapy or another type of intravenous (IV) chemotherapy can be substituted. Radiation therapy is given five days per week. This combination probably works as well as the chemotherapy pump plus radiation therapy, although formal studies comparing the two approaches have not been done.
Treatment of stage IV (metastatic) disease — For patients who are initially diagnosed with metastatic pancreatic cancer (stage IV), chemotherapy might be recommended to slow the spread of the cancer and relieve symptoms.
Chemotherapy does not cure metastatic pancreatic cancer, but it can relieve symptoms, slow disease progression, and prolong life. Talk to your doctor about the benefits and risks of chemotherapy. Your doctor might suggest participating in a clinical trial that compares new chemotherapy medicines or new combinations of treatment.
Treating pancreatic cancer symptoms — Pancreatic cancer often causes bothersome symptoms like jaundice, intestinal blockage, pain, and weight loss. Treatments are available to relieve these symptoms.
Jaundice — Jaundice is caused by a blockage of the flow of bile from the gallbladder into the intestine. The most common treatment is a stent, which is a small tube that is inserted into a duct to keep it open. The stent can usually be placed in a procedure called ERCP (endoscopic retrograde cholangiopancreatography). More information on this procedure is available separately.
Intestinal blockage — Some patients with pancreatic cancer will develop a blockage in the upper intestine (duodenum) caused by the tumor. Surgery can be done to create a detour between the stomach and a lower part of the intestine. An alternative to bypass surgery is placement of a stent (tube) in the duodenum. The stent helps to hold open the blocked area.
Pain — Pain is a common problem in people with pancreatic cancer. In some people, prescription pain medicine alone is all that is needed. Radiation therapy can also help relieve pain by shrinking the tumor.
A procedure called "celiac plexus block" might also be a good option to control pain. This procedure uses injections of alcohol into nerves that transmit pain signals. The alcohol kills the nerves, preventing them from telling the brain to feel pain.
Weight loss — Weight loss is common in people with pancreatic cancer. Taking a pancreatic enzyme replacement can help your body to absorb fat. Enzyme replacements are usually taken in a capsule on a daily basis.
If nausea and vomiting are a problem, there are several medicines that can reduce these symptoms and improve the appetite.
ADVANCED CANCER AND END OF LIFE CARE — In many people with pancreatic cancer, the disease cannot be cured. Deciding when to stop treating the cancer can be difficult, and the decision should involve the patient, family, friends, and the healthcare team.
Ending cancer treatment does not mean ending care for the patient. Hospice care is frequently recommended when a person is unlikely to live longer than six months. Hospice care involves treatment of all aspects of a patient and family's needs, including the physical (eg, pain relief), psychological, social, and spiritual aspects of suffering. This care may be given at home or in a nursing home or hospice facility, and usually involves multiple care providers, including a physician, registered nurse, nursing aide, a chaplain or religious leader, a social worker, and volunteers.
These providers work together to meet the patient and family's needs and significantly reduce their suffering. For more information about hospice, seewww.hospicenet.org.
INTRODUCTION — The pancreas is an organ that is located behind the stomach. Its normal function is to make hormones that regulate glucose (blood sugar) levels and produce digestive juices that help the body break down food.
More than 42,000 Americans develop cancer of the pancreas each year; it is the fourth leading cause of cancer-related death in the United States. Two types of cancer can affect the pancreas:
●The most common is cancer of the exocrine pancreas that originates in the pancreatic ducts. The ducts are responsible for carrying pancreatic juice to the intestines. This type of pancreatic cancer, called "pancreatic ductal adenocarcinoma," is discussed in this article.
●Another type of cancer consists of a group of tumors that originate from the cells that make hormones such as insulin. These tumors are called "pancreatic endocrine tumors," and are not discussed here.
PANCREATIC CANCER SYMPTOMS — Most people with pancreatic cancer have pain and weight loss, with or without jaundice (yellowing of the skin):
●Pain – Pain is a common symptom. It usually develops in the upper abdomen as a dull ache that wraps around to the back. The pain can come and go, and it might get worse after eating.
●Weight loss – Some people lose weight because of a lack of appetite, feeling full after eating only a small amount of food, or having diarrhea. The bowel movements might look greasy and float in the toilet bowl because they contain undigested fat.
●Jaundice – This causes yellow colored skin and whites of the eyes. Bowel movements may not be a normal brown color and instead have a grayish appearance. Jaundice is caused by a block in the flow of bile from the gallbladder, where it is stored, to the intestinal tract where the bile assists in digestion of food. The block is caused by the cancer.
PANCREATIC CANCER DIAGNOSIS — If you develop symptoms that raise suspicion for pancreatic cancer, your doctor or nurse will order one or more tests. These might include blood tests and imaging tests, such as an ultrasound or computed tomography (CT) scan, and/or an endoscopic test called endoscopic retrograde cholangiopancreatography (ERCP).
These tests can show if there is a mass (growth) in the pancreas and if surgery to remove the mass is possible.
Biopsy — In some cases, your doctor will recommend a biopsy to confirm the diagnosis of cancer. A biopsy involves removing a small piece of tissue from the mass. A physician examines the tissue under a microscope to see if there are signs of cancer.
To perform the biopsy, a doctor will use a CT scan or ultrasound to pinpoint the location of the mass, then insert a needle into the mass and take a sample of tissue. A biopsy may also be obtained using ERCP or a different type of endoscopic procedure called endoscopic ultrasound (EUS).
PANCREATIC CANCER STAGING — Once pancreatic cancer is diagnosed, the next step is to determine its stage. Staging is a system used to describe the aggressiveness and spread of a cancer. A pancreatic cancer's stage is based on:
●The size of the cancer
●If there are signs of cancer spread outside the pancreas on a physical exam, computed tomography (CT) scan or magnetic resonance imaging (MRI), chest x-ray, or other imaging tests
The staging of a pancreatic cancer often depends not only on imaging studies, but also on what is found during surgery.
Pancreatic cancer stages range from stage I, the earliest stage, to stage IV, which means that the cancer has spread to distant organs (such as the liver). In general, lower stage cancers are more likely to be successfully treated than are higher stage cancers. Most physicians who care for patients with pancreatic cancer refer to patients as having surgically resectable cancer (stage I and II), locally advanced cancer (stage III), or metastatic cancer (stage IV).
Sometimes you will hear physicians describe a stage that technically doesn’t exist called "borderline resectable." This occurs because some locally advanced cancers can be resected completely, but many cannot. Imaging doesn’t always accurately distinguish between the two. In such cases, chemotherapy, with or without radiation therapy, might be used initially to attempt to shrink the tumor and increase the chance that it might become resectable.
Laparoscopy — In some centers, a laparoscopy is recommended before an attempt to remove the cancer surgically to get more information about the location and size of the cancer. During a laparoscopy, a surgeon inserts a thin tube with a camera into small incisions in the belly to see the organs inside the abdomen.
PANCREATIC CANCER TREATMENT — Pancreatic cancer can be treated with several approaches. Early stage pancreatic cancer can often be treated and even cured with surgery. After surgery, further treatment, called "adjuvant therapy," is often recommended. This might include chemotherapy or radiation therapy.
However, surgery is often not possible; pancreatic cancer is often advanced by the time it is diagnosed. If surgery is not possible, radiation therapy, chemotherapy, or both are often used to shrink the cancer, reduce symptoms, and prolong life.
Surgery for tumors in the head of the pancreas — The standard operation for tumors in the head of the pancreas is a Whipple procedure (also called a pancreaticoduodenectomy).
In this procedure, the surgeon removes the pancreatic head, the duodenum (the first part of the small intestine), part of the jejunum (the next part of the small intestine), the common bile duct, the gallbladder, and part of the stomach. A modification of the Whipple procedure (called a "pylorus-preserving" Whipple procedure) has been developed that preserves the part of the stomach (the pylorus) that is important for stomach emptying.
In the past, complications and deaths following the Whipple procedure were high, and cure rates were less than 10 percent. However, more recent results suggest better outcomes. Better outcomes are more likely in hospitals that perform a large number of Whipple procedures and when the surgeon is experienced with the procedure.
Surgery for tumors in the body or tail of the pancreas — Because tumors in the body or tail of the pancreas do not cause the same symptoms as those in the head of the pancreas, these cancers tend to be discovered at a later stage, when they are more advanced.
If the tumor can be removed with surgery, a laparoscopy is usually done first to make sure the cancer has not spread. If surgery is an option, part of the pancreas is removed, usually along with the spleen.
Adjuvant therapy after surgery — Adjuvant (additional) therapy refers to chemotherapy, radiation, or a combination of both. Adjuvant therapy is recommended for people who are thought to be at high-risk of having cancer reappear (termed a recurrence or a relapse) after a tumor has been removed surgically.
Even if the tumor has been completely removed, tiny cancer cells may remain in the body and grow, causing relapse after surgery. Adjuvant therapy can prolong survival by eliminating the tiny cancer cells before they have a chance to grow.
In people with completely resected pancreatic cancer, there are two ways to give adjuvant therapy after surgery:
●Give chemotherapy alone
●Give a combination of chemotherapy and radiation therapy (this strategy is called "chemoradiotherapy")
In the United States, after successful surgical removal of a pancreatic cancer, chemoradiotherapy is recommended for many patients, although chemotherapy alone is increasingly used. Outside of the United States, patients are frequently offered chemotherapy alone.
Treatment of locally advanced pancreatic cancer — Locally advanced pancreatic cancer refers to a situation in which the cancer has not yet spread to distant locations in the body, but it has extended into areas around the pancreas that make it difficult or impossible to remove the tumor completely. As determined by imaging studies (typically computed tomography [CT] and magnetic resonance imaging [MRI] scans), some of these cases may be classified as "borderline" resectable, while others are locally advanced and not resectable, according to standard guidelines.
The best treatment for locally advanced pancreatic cancer is not clear, but surgery is not usually offered initially. Options for treatment include chemotherapy alone or chemotherapy followed by a combination of chemotherapy and radiation therapy (chemoradiotherapy). In some cases, these treatments may be followed by repeat imaging and surgical exploration to see if tumor removal might be possible. Ideally, patients with locally advanced pancreatic cancer should be offered treatment as part of a clinical trial testing the benefit of new treatment strategies.
Chemoradiotherapy — Chemoradiotherapy often requires a central venous access catheter (often called a "port"). This is a tube that is surgically inserted into one of the large blood vessels in the chest. Chemoradiotherapy often requires a portable chemotherapy pump; this is a small, battery-operated pump that fits into a pack that can be worn around the waist. The pump gives the chemotherapy medicine into the port continuously for five to six weeks.
During this time, the patient is treated with radiation therapy five days per week. The radiation is delivered while the patient lies on a table underneath or in front of the machine. The treatment takes only a few seconds (similar to having an X-ray).
Sometimes the chemotherapy pump is not covered by health insurance. In this case, an oral (pill) form of chemotherapy or another type of intravenous (IV) chemotherapy can be substituted. Radiation therapy is given five days per week. This combination probably works as well as the chemotherapy pump plus radiation therapy, although formal studies comparing the two approaches have not been done.
Treatment of stage IV (metastatic) disease — For patients who are initially diagnosed with metastatic pancreatic cancer (stage IV), chemotherapy might be recommended to slow the spread of the cancer and relieve symptoms.
Chemotherapy does not cure metastatic pancreatic cancer, but it can relieve symptoms, slow disease progression, and prolong life. Talk to your doctor about the benefits and risks of chemotherapy. Your doctor might suggest participating in a clinical trial that compares new chemotherapy medicines or new combinations of treatment.
Treating pancreatic cancer symptoms — Pancreatic cancer often causes bothersome symptoms like jaundice, intestinal blockage, pain, and weight loss. Treatments are available to relieve these symptoms.
Jaundice — Jaundice is caused by a blockage of the flow of bile from the gallbladder into the intestine. The most common treatment is a stent, which is a small tube that is inserted into a duct to keep it open. The stent can usually be placed in a procedure called ERCP (endoscopic retrograde cholangiopancreatography). More information on this procedure is available separately.
Intestinal blockage — Some patients with pancreatic cancer will develop a blockage in the upper intestine (duodenum) caused by the tumor. Surgery can be done to create a detour between the stomach and a lower part of the intestine. An alternative to bypass surgery is placement of a stent (tube) in the duodenum. The stent helps to hold open the blocked area.
Pain — Pain is a common problem in people with pancreatic cancer. In some people, prescription pain medicine alone is all that is needed. Radiation therapy can also help relieve pain by shrinking the tumor.
A procedure called "celiac plexus block" might also be a good option to control pain. This procedure uses injections of alcohol into nerves that transmit pain signals. The alcohol kills the nerves, preventing them from telling the brain to feel pain.
Weight loss — Weight loss is common in people with pancreatic cancer. Taking a pancreatic enzyme replacement can help your body to absorb fat. Enzyme replacements are usually taken in a capsule on a daily basis.
If nausea and vomiting are a problem, there are several medicines that can reduce these symptoms and improve the appetite.
ADVANCED CANCER AND END OF LIFE CARE — In many people with pancreatic cancer, the disease cannot be cured. Deciding when to stop treating the cancer can be difficult, and the decision should involve the patient, family, friends, and the healthcare team.
Ending cancer treatment does not mean ending care for the patient. Hospice care is frequently recommended when a person is unlikely to live longer than six months. Hospice care involves treatment of all aspects of a patient and family's needs, including the physical (eg, pain relief), psychological, social, and spiritual aspects of suffering. This care may be given at home or in a nursing home or hospice facility, and usually involves multiple care providers, including a physician, registered nurse, nursing aide, a chaplain or religious leader, a social worker, and volunteers.
These providers work together to meet the patient and family's needs and significantly reduce their suffering. For more information about hospice, seewww.hospicenet.org.